Provide the definition of public health nutrition (PHN) given by the Academy of Nutrition and Dietetics Public Health Nutrition Task Force in 2012.
Explain five key roles of a public health nutritionist within a public health agency.
Describe the Social-Ecological Model and how it can be used by public health nutritionists to understand the multiple levels of influence on nutrition- and other health-related behaviors.
Describe the core functions of public health including assessment, assurance, and policy development.
List the 10 essential public health services and 16 essential public health nutrition services that support these core functions.
Describe essential areas of training for public health nutritionists, including advanced training in nutrition and public health, knowledge of current nutrition-related evidence-based skills, and the core functions of public health.
INTRODUCTION
History of PHN in the United States
Mary Egan,1 a leader in shaping contemporary PHN education and practice in the United States, delineated the history of PHN with major milestones that influenced its development from the mid-1800s to the mid-1990s. During the mid-1800s, which was described as the “great sanitary awakening,”2 the modern public health system (Figure 1.1)3 began with a focus on sanitation efforts to decrease the spread of communicable diseases.4 At this time, PHN was in its infancy with origins in home economics and public health and a focus on food safety and meal preparation on a budget. In the early 1900s, morbidity and mortality rates were high, especially among the working poor, infants, children, and mothers. In 1906, the Food and Drug Act was passed by Congress to begin oversight of food production, sales, and labeling.4 In 1909, under the leadership of President Theodore Roosevelt, the White House held its first conference, the White House Conference on the Care of Dependent Children.5 Because of this conference, the Children’s Bureau was created, which in effect launched the field of PHN.1 The Sheppard–Towner Act in 1921 and the Social Security Act in 1935 had profound influences on public health infrastructure and the subsequent growth of PHN. Funds available to state health departments for maternal and child health through Title V of the Social Security Act stimulated rapid growth in the field. Prior to 1935, only three public health nutritionists were employed in three states, but by 1939, 39 public health nutritionists were employed in 24 states. In 1938, public health nutritionists’ qualifications were first delineated. The Social Security Act was amended in 1939, and funds were available to train public health nutritionists. In 1942, based in part on nutrition studies conducted by the Public Health Service, nutrition clinics were developed in some state and local public health agencies. By the mid-1940s, 45 of the 48 states employed one or more PHN consultants, and funding to train graduate students in PHN and provide continuing education for practicing PHN professionals was allocated.1
During the 1950s, growth of the profession became more organized with the establishment of the Association of Faculties of Graduate Programs in Public Health Nutrition (currently, the Association of Graduate Programs in Public Health Nutrition)6 in 1950 and the Association of State and Territorial Public Health Nutrition Directors (currently, the Association of State Public Health Nutritionists) in 1952. In the mid-1960s, legislation passed to reduce poverty in the United States provided funding for projects like the Maternity and Infant Care Program, the Compressive Health Projects for Children and Youth, Head Start, and the Medicare and Medicaid programs. These programs opened many more positions for public health nutritionists as practitioners in the programs or as consultants. The 1969 White House Conference on Food, Nutrition, and Health suggested actions to reduce malnutrition and hunger.7 One of the recommendations was to provide nutrition services to pregnant women, infants, and young children from impoverished households. In 1972, the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) began as a pilot program, and in 1975, it was funded as a permanent nutrition education and supplemental food program.8 To assess the nutrition status of the population, the Children’s Bureau and the Public Health Service began collecting data in the late 1960s and early 1970s via the Study of Nutritional Status of Preschool Children in the United States,9 the Ten State Survey, 1968-1970,10 and the National Health and Nutrition Examination Survey, 1971-1975.11 These programs and studies expanded positions and the scope of practice of public health nutritionists.1
In the 1970s and 1980s, several landmark documents were released that focused on the importance of nutrition in the prevention of chronic diseases and to provide dietary guidance for the U.S. population. First, in 1977, the Dietary Goals for the United States12 were released, followed by Healthy People: The Surgeon General’s Report on Health Promotion and Disease Prevention in 1979,13 which outlined the first set of national health goals and objectives that focused on health promotion and disease prevention and highlighted the role of nutrition in these areas. The next year, two important documents were released. First, Promoting Health/Preventing Disease: Objectives for the Nation was released13 and included 226 health-related objectives and action steps for improving population health over the next decade. These documents were the forerunners for the Healthy People series of documents,14 which are science-based health objectives for the U.S. population that are released every 10 years. The second landmark document released that year was Nutrition and Your Health: Dietary Guidelines for Americans.15 This was the first edition of dietary guidance for the U.S. population that focused on healthful dietary patterns based on the most accurate scientific evidence at the time.16
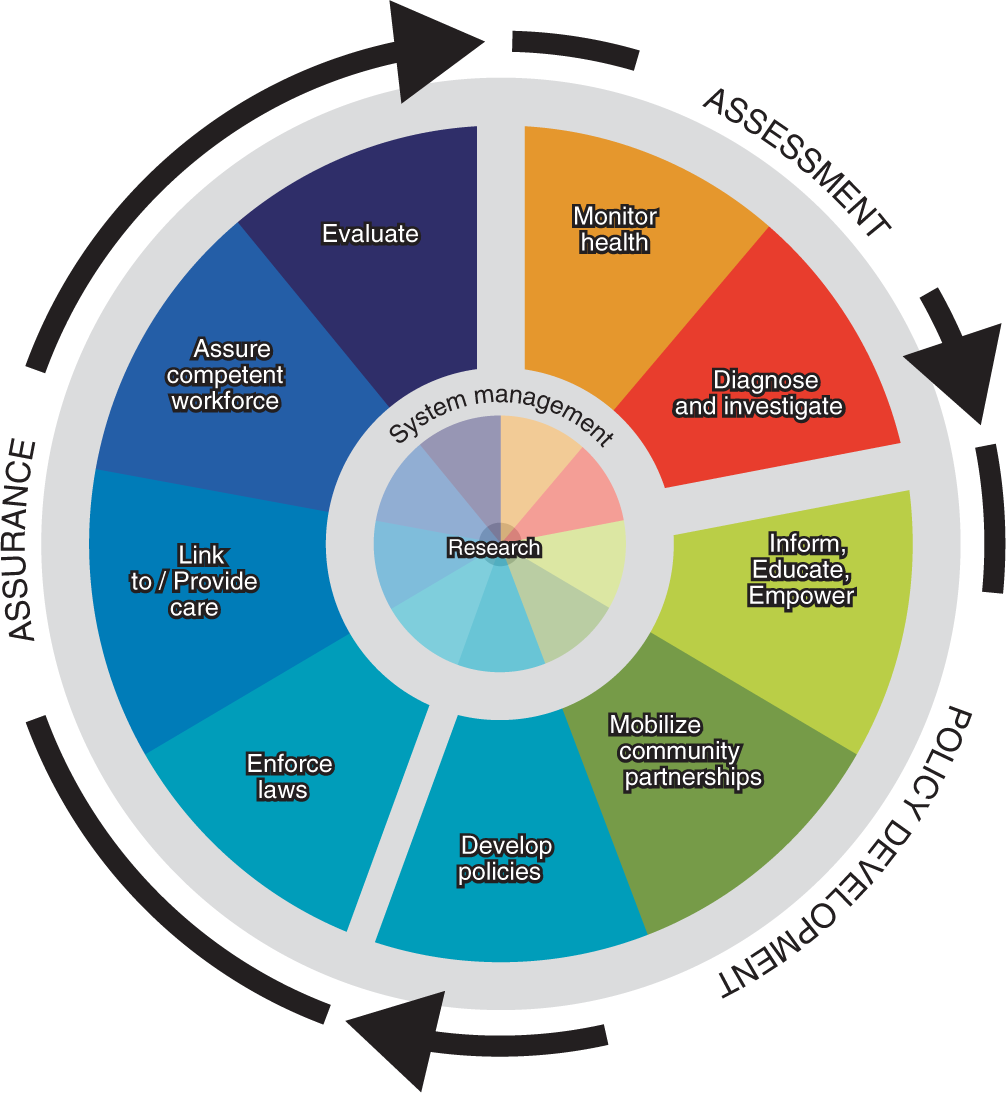
During the past two decades of the 1900s, as scientific understanding of chronic diseases and their relationship to nutrition continued to develop, public health nutritionists began working across the life course in the areas of health promotion and disease prevention. The Centers for Disease Control and Prevention (CDC) established the National Center for Chronic Disease Prevention and Health Promotion in 1988 and expanded the roles of public health nutritionists at the federal level working with states and other agencies to decrease chronic disease.17 Also, in 1988, the Institute of Medicine (IOM) released a groundbreaking document, The Future of Public Health.4,18 This document outlined the three core functions of public health—assessment, policy development, and assurance—and the 10 essential services of public health (Figure 1.2).19 In 1996, the book, Moving to the Future: Developing Community-Based Nutrition Services20 delineated the essential PHN services, which are still relevant today based on a recent article that defined a similar list of core functions of the PHN workforce in Australia.21 Table 1.1 delineates the essential PHN services, as outlined by Probert, in relationship to the core functions of public health.
The Healthy People14 series of national health objectives began with Healthy People 2000,22 released September 1990. Since the introduction of these national health objectives, major progress has been made in the reduction of preventable illness and death, including nutrition-related diseases, cardiovascular disease, and cancer, along with risk factors such as hypertension and hyperlipidemia.23 However, there is much work to be done still. Two nutrition-related leading health indicators, “reduce the proportion of adults who are obese” and “reduce the proportion of children and adolescents aged 2 to 19 years who are considered obese,” have not met the 2020 targets and have actually increased from 33.9% to 38.6% and 16.1% to 17.8%, respectively. Healthy People 2020 objectives related to dietary intake need improvement as well. Although these objectives have improved from baseline, National Health and Nutrition Examination Survey (NHANES) data show that for the U.S. population, the mean daily intake of vegetables is still below the national objective of 1.6 cup equivalents per 1,000 calories (age-adjusted) and mean percentage of total daily calorie intake from added sugars (age-adjusted) and mean daily sodium intake (age-adjusted) are above the objectives of 9.7% and 2,300 mg, respectively. Healthy People 2030,24 the newest edition of the Healthy People series, has seven foundation principles, five overarching goals, and eight action areas (Box 1.1). With a continued focus on prevention of chronic diseases, public health nutritionists will continue to play vital roles in improving population health.
GLOBAL PHN
Global PHN practice and services are much more recent concepts than PHN practice and services in developed nations. Like the United States, developed, transitioning, and developing countries have their own unique histories related to the foundations of public health and, subsequently, the growth of PHN. From the mid-1990s until now, international dietary intake patterns and physical activity levels and sedentary behaviors changed rapidly as a result of greater industrialization, changes in the world food economy, technology, and globalization.25 Because of these dietary intake and activity changes, there was an ensuing increase in nutrition-related chronic diseases; poorer communities, especially in developing and newly developed countries, experience a disproportionate burden of morbidity and mortality from chronic diseases such as diabetes, cardiovascular disease, and cancer.26 Like most official health agencies, the World Health Organization (WHO), created in 1948 as part of the United Nations, was formed to combat communicable diseases and to improve maternal, infant, and child health and nutrition.27 Now, WHO is the most prominent health agency in the world and assists public health agencies around the globe in responding to both communicable and noncommunicable diseases.
TABLE 1.1
PUBLIC HEALTH CORE FUNCTIONS AND ESSENTIAL PUBLIC HEALTH NUTRITION SERVICES
| PUBLIC HEALTH CORE FUNCTION(S) | ESSENTIAL PUBLIC HEALTH NUTRITION SERVICES |
|---|
| Assessment | Assessing the nutritional status of specific populations or geographic areas |
| Identifying priority populations that may be at nutritional risk |
| Initiating and participating in nutrition data collection |
| Policy development | Providing leadership in the development of and planning for health and nutrition policies |
| Raising awareness among key policy-makers on the potential impact of nutrition and food regulations on budget decisions on the health of the community |
| Acting as an advocate for priority populations on food and nutrition issues |
| Assurance | Planning for nutrition services in conjunction with other health services, based on information obtained from an adequate and ongoing database focused on health outcomes |
| Recommending and providing specific training and programs to meet identified nutrition needs |
| Identifying or assisting in development of accurate, up-to-date nutrition education materials |
| Ensuring the availability of quality nutrition services to priority populations, including nutrition screening, assessment, education, counseling, and referral for food assistance and follow-up |
| Providing community health promotion and disease prevention activities that are population-based |
| Providing quality assurance guidelines for practitioners dealing with food and nutrition issues |
| Facilitating coordination with other providers of health and nutrition services within the community |
| Assessment/Assurance/Policy development | Participating in nutrition research, demonstration, and evaluation projects |
| Providing expert nutrition consultation to the community |
| Evaluating the impact of the health status of populations who receive public health nutrition services |
BOX 1.1
HEALTHY PEOPLE 2030 FOUNDATION PRINCIPLES, OVERARCHING GOALS, AND PLAN OF ACTION
Foundational Principles
Health and well-being of all people and communities are essential to a thriving, equitable society.
Promoting health and well-being and preventing disease are linked efforts that encompass physical, mental, and social health dimensions.
Investing to achieve the full potential for health and well-being for all provides valuable benefits to society.
Achieving health and well-being requires eliminating health disparities, achieving health equity, and attaining health literacy.
Healthy physical, social, and economic environments strengthen the potential to achieve health and well-being.
Promoting and achieving the nation’s health and well-being is a shared responsibility that is distributed across the national, state, tribal, and community levels, including the public, private, and not-for-profit sectors.
Working to attain the full potential for health and well-being of the population is a component of decision-making and policy formulation across all sectors.
Overarching Goals
Attain healthy, thriving lives and well-being, free of preventable disease, disability, injury, and premature death.
Eliminate health disparities, achieve health equity, and attain health literacy to improve the health and well-being of all.
Create social, physical, and economic environments that promote attaining full potential for health and well-being for all.
Promote healthy development, healthy behaviors, and well-being across all life stages.
Engage leadership, key constituents, and the public across multiple sectors to take action and design policies that improve the health and well-being of all.
Plan of Action
Set national goals and measurable objectives to guide evidence-based policies, programs, and other actions to improve health and well-being.
Provide data that is accurate, timely, accessible, and can drive targeted actions to address regions and populations with poor health or at high risk for poor health in the future.
Foster impact through public and private efforts to improve health and well-being for people of all ages and the communities in which they live.
Provide tools for the public, programs, policy-makers, and others to evaluate progress toward improving health and well-being.
Share and support the implementation of evidence-based programs and policies that are replicable, scalable, and sustainable.
Report biennially on progress throughout the decade from 2020 to 2030.
Stimulate research and innovation toward meeting Healthy People 2030 goals and highlight critical research, data, and evaluation needs.
Facilitate development and availability of affordable means of health promotion, disease prevention, and treatment.
Source: From U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. Healthy People 2030 Framework. 2019, November 4. https://www.healthypeople.gov/2020/about-healthy-people/development-healthy-people-2030/framework
PHN: DEFINITIONS
Several organizations have made efforts to define PHN and public health nutritionist for the past several decades.28–32 PHN professionals and academicians in the United States, the United Kingdom, Australia, and Canada, as well as other countries in the European Union, have worked separately and together to develop working definitions of PHN. One of the first formal definitions of public health nutritionist in the United States was provided by Margaret Kaufmann in Personnel in Public Health Nutrition in the 1980s as
that member of the public health agency staff who is responsible for assessing community nutrition needs and planning, organizing, managing, directing, coordinating, and evaluating the nutrition component of the health agency’s services … establishes linkages with related community nutrition programs, nutrition education, food assistance, social or welfare services, child care, services to the elderly, other human services, and community-based research.32
Hughes,33 an international PHN workforce development researcher, called for a standard definition of PHN among a working group from nine countries so that that workforce requirements could be assessed internationally. The international work group recommended various key descriptors from various aspects of the profession so that each country could develop its own definition that was best suited to the core functions and services that were unique to each country. The key descriptors to define PHN were “solution-oriented, social and cultural aspects, advocacy, disease prevention, and interventions based on systems, communities and organizations.”33
In the ensuing years, definitions of PHN were formalized by several organizations and authors. Table 1.2 outlines organizations’ definitions of PHN since 1998. As seen, there are commonalities among the PHN definitions and for the scope of practice of PHN professionals, for example, advocating for a healthful environment for all; developing policies based on system- and population-level assessments and program evaluations in priority populations; and collaborating with key stakeholders to improve programs, services, and policies. Regardless of the definition used for PHN, the similarity of ideas is central to the distinct differentiation between PHN practice and clinical nutrition practice. Thus, these definitions indicate that PHN professionals should have advanced training in nutrition and public health to develop an in-depth knowledge of the most up-to-date nutrition-related evidence base and competencies and skills related to the core public health functions and the essential services of public health and PHN.
TABLE 1.2
DEFINITIONS OF PUBLIC HEALTH NUTRITION BY ORGANIZATION AND DATE
| ORGANIZATION | DATE | DEFINITION |
|---|
| United Kingdom Nutrition Society | 1998 | The application of nutrition and physical activity to the promotion of good health, the primary prevention of diet-related illness of groups, communities, and populations (not individuals)34 |
| Strategic Intergovernmental Nutrition Alliance (Australia) | 2001 | Focuses on issues affecting the whole population rather than the specific dietary needs of individuals The impact of food production, distribution, and consumption on the nutritional status and health of particular population groups is taken into account, together with the knowledge, skills, attitudes, and behaviors in the broader community35 |
| World Public Health Nutrition Association | 2006 | The promotion and maintenance of nutrition-related health and well-being of populations through organized efforts and informed choices of society31 |
| Dietitians of Canada | 2006 | Health promotion through awareness raising, education and skill building, supportive environments and policy development, collaborations and partnerships, research and evaluation, and the mentoring and education of future nutrition and health professionals as well as other congruent descriptors29 |
| Academy of Nutrition and Dietetics PHN Task Force | 2012 | The application of nutrition and public health principles to improve or maintain optimal health of populations and targeted groups through enhancements in programs, systems, policies, and environments28 |
PHN: TRAINING AND WORKFORCE
In recent years, PHN has received more attention and greater research funding owing to problems both domestically and globally related to the obesity epidemic, chronic diseases, and food insecurity.36 As the U.S. population and populations in other developed countries continue to get older and become more diverse, population needs and public health and clinical healthcare, including nutrition, will need to adjust. Longer life spans increase the duration of chronic diseases and rate of comorbidities, which increase the necessity of lifestyle interventions that target culturally appropriate nutrition and physical activity behaviors. Further, because of economic hardships in recent years, food assistance programs, such as the Supplemental Nutrition Assistance Program (SNAP, formerly the Food Stamp Program) and WIC, have had some of the greatest utilization rates in years. Because these programs are often targeted by proposed budget cuts, many Americans, especially low-income and other disenfranchised populations, may be at increased risk for nutrition-related chronic diseases. In the United States and globally, it is essential to have highly trained PHN practitioners who can meet the needs of these populations and advocate for positive nutrition-related health outcomes for vulnerable populations across the life course.28,36,37 PHN practitioners’ knowledge and skills are essential to improving population health; they are essential members of interprofessional public health teams and assist with policy- and system-level decisions for health promotion and disease prevention.37 Public health nutritionists’ competencies are particularly important now; the Patient Protection and Affordable Care Act38 underscores the need for primary prevention as well as screening and treatment of chronic diseases.39
The IOM40 delineated recommendations for training public health professionals, the myriad of health concerns, and the essentiality of multidisciplinary and interdisciplinary/interprofessional approaches in Who Will Keep the Public Healthy? Educating Public Health Professionals for the 21st Century. The document asserts that to improve the nation’s health, all members of multidisciplinary/interdisciplinary/interprofessional teams must be well trained and use evidence-based guidelines and best practices. It is essential that public health nutritionists have the competencies needed to help curtail obesity epidemic rates and decrease rates of other nutrition-related chronic diseases. Thus, PHN training should include in-depth exposure to the Social-Ecological Model,41 along with other behavioral theories, and the social determinants of health because it is essential for public health nutritionists to understand how behavioral, environmental, biological, societal, and economic factors influence individual health and, subsequently, population health.37,42 Further, training in PHN should include applied nutrition science; nutrition across the life course; policy development, implementation, and evaluation; biostatistics; epidemiology; public policy related to nutrition and food assistance; community assessment; and program planning, implementation, and evaluation.43
PHN: POSITIONS AND CAREER SETTINGS
Position descriptions, classifications, educational requirements, and career settings for PHN practitioners are outlined in Personnel in Public Health Nutrition for the 2000s.44 In this document, PHN professionals are described as “specialized nutrition professionals and paraprofessionals who provide and/or plan nutrition programs through organizations that reach people living in a designated community”.44 PHN professionals may be employed in numerous career settings at state, local, and national agencies and organizations in both the public and private sectors. In addition to local and state public health agencies, other common places that employ or contract with PHN practitioners include federally qualified community health clinics, nonprofit organizations, state departments of education, food assistance programs, hunger-relief agencies, early childhood education settings such as Head Start, and local education agencies, where they are employed as nutrition educators, school health coordinators, or directors of nutrition services. In addition, public health nutritionists work in federally sponsored programs at the local level, such as WIC, SNAP-Ed, and the Expanded Food and Nutrition Education Program, and many federal agencies such as the U.S. Department of Health and Human Services, the U.S. Department of Agriculture, the CDC, Food and Drug Administration, Maternal and Child Health Bureau, and Indian Health Services. Although this list is not all inclusive, it does show the variety of job settings for PHN personnel.
FIGURE 1.3
The Social-Ecological Model.

Source: Data from U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion. The 2015-2020 Dietary Guidelines. The Social-Ecological Model. 2015. https://health.gov/dietaryguidelines/2015/guidelines/chapter-3/social-ecological-model; Centers for Disease Control and Prevention. The Social Ecological Model: A Framework for Prevention. 2019, January. http://www.cdc.gov/violenceprevention/overview/social-ecologicalmodel.html; World Health Organization. Violence Prevention Alliance. The Ecological Framework. 2019. https://www.who.int/violenceprevention/approach/ecology/en.; Bronfenbrenner U. Toward an experimental ecology of human development. Am Psychol. 1977;32(7):513–531. doi:10.1037/0003-066X.32.7.513
PHN positions can be classified across a continuum of services and functions from direct care services to population and systems focused work.44 To influence individual and population health, professionals in PHN work across the spheres of influence in the Social-Ecological Model (Figure 1.3).41,45,46,58 However, most often, these practitioners focus on the outer spheres at the societal and policy levels and within sectors and organizations. Personnel in management positions, which include directors, assistant directors, and supervisors, work predominantly in administrative roles and have little direct contact with their priority populations. Public health nutritionists, consultants, clinical nutritionists, nutritionists, and nutrition educators are classified as professional positions. While public health nutritionists and consultants may have some direct interactions with community members, much of their work is in program planning, implementation, and evaluation. Other professional positions, including clinical nutritionists, nutritionists, and nutrition educators, along with positions classified as technical and support positions, such as nutrition technicians and community nutrition workers, usually have direct contact with the public with a focus on delivery of services. Personnel at the management level and public health nutritionists and consultants at the professional level require advanced training in public health and nutrition so that they are competent in community assessment; are able to plan, implement, and evaluate population- and systems-level programs and services; and have the knowledge and skills required to collaborate and lead interprofessional teams to promote population health.44
According to the U.S. Bureau of Labor Statistics,47 career growth in nutrition and dietetics is projected to increase over the next decade by 11%, which is higher than growth in many other professions. Job growth in PHN may increase even more if the healthcare system continues to shift from a medical treatment model to one of primary prevention.39 In 2018, the average pay for dietitians/nutritionists was $64,670 annually, with higher paying positions in states on the West Coast and in large metropolitan areas.47
PHN: FUTURE TRENDS
In 2006, the World Congress of PHN, an international association of PHN practitioners, academicians, researchers, clinical and public health professionals, policy-makers, and epidemiologists from 79 countries, convened a discussion session to examine the future trends and educational needs of PHN professionals nationally, regionally, and globally.48 The panel outlined a global need for research, improved technology, and strong collaborations between academia and both private and public sectors to find solutions to malnutrition, both under- and overnutrition, and other nutrition-related health problems. The panel recommended that multiple disciplines from both developed and developing countries should collaborate to find solutions to the global problems, similar to how multinational, multidisciplinary teams have worked to eliminate or dramatically reduce communicable diseases via immunization. Also, the panel recommended that once formed, the collaborations would need to be guided by shared ethical principles, transparency, and open communication. Thus far, such collaborations have been limited, but in May 2008, based on recommendations from the World PHN Congress, the World Association of PHN was incorporated.49 The purpose of the association is to bring people together to promote and improve PHN and to be the international voice of PHN.
Because current PHN professionals must work to meet the nutrition-related needs of the public to promote population health through nutrition services, interventions, initiatives and policy, systems, and environmental change, it is important that this workforce be trained through graduate coursework and experiential learning and, after entry into the workforce via continuing education, have opportunities for leadership development and other professional development training.50 Hughes,31 in an editorial about PHN workforce development, outlined key areas that should be examined to increase the capacity and quality of highly trained PHN professionals, including increased scholarship for the PHN workforce, strong assessment to determine workforce needs, in both developing and developed nations, and funding to conduct such research and train the workforce. Shrimpton et al.50 noted that development of workforce capacity in PHN should be assessed at each of the following levels: in the PHN workforce, within communities, and at organizational and systems levels.
Currently, PHN workforce development needs are addressed via multiple training avenues, including online certificate training, such as the Academy of Nutrition and Dietetics Center for Lifelong Learning Public Health Nutrition Online Certificate Training;51 academic graduate certificate programs, such as Appalachian State University Graduate Certificate in Public Health Nutrition Practice;52 academic coursework in nutrition and public health; graduate programs in PHN and community nutrition;6 and certification programs, for example, Certification in Public Health53 and Certified Health Education Specialist.54 Although an undergraduate degree in nutrition is necessary and advanced education at the graduate level and the registered dietitian/nutritionist credential is preferred, currently there is no specific credential or licensure available to denote a professional’s advanced training in PHN. Thus, some public health nutritionists may not have the advanced training and competencies to adequately perform their role. Without advanced training and practice, PHN professionals may be ill-prepared to carry out the core functions of public health and the essential PHN services and work at the system, population, and community levels.29 Thus, in the future to protect population health, all public health nutritionists should have graduate-level PHN coursework and/or degrees to ensure that the workforce is competent in the areas of community nutrition assessment; program planning, implementation, and evaluation; policy development, implementation, and evaluation; and policy systems and environmental change.29,37,43
Another key area of future focus for the PHN workforce is leadership development to ensure organization-, community-, policy-, and systems-level competencies to promote health and prevent nutrition-related diseases for populations.55 The current workforce in PHN is aging;56 this will lead to many retirements and the absence of PHN practitioners in leadership roles in the profession.55,56 Thus, future demands on the PHN workforce must be addressed to help close these gaps. Leadership development is and will continue to be imperative to the PHN profession, as it will allow entry- and midlevel career personnel in PHN to be better equipped to fill vacant leadership positions in public health and PHN and mentor students, trainees, and interns in the field.57 Because the number of PHN practitioners needed domestically and globally may take several decades to reach the capacity to serve population needs, increased graduate programs in PHN and continuing education for current practitioners are necessary.50
Closely aligned with leadership development, developing skilled mentors will also be key to increasing the capacity of the PHN workforce in the future. Palermo et al.,57 Australian advocates for and researchers on PHN workforce development, recommended the development of PHN mentoring circles, that is, pairing an experienced PHN professional with a group of entry-level PHN practitioners. This could increase each mentor’s capacity and effectiveness. Although the effectiveness of these mentoring circles would depend on the commitment, significance, and involvement of everyone in the group, it could be a valid solution to the shortage of experienced PHN practitioners who can assist in the development of new PHN practitioners and leaders.
CONCLUSION
PHN has a rich history of improving population health and a challenging, ambitious, and exciting future in decreasing nutrition-related health disparities, ensuring access to food, and improving the health status of populations across the globe. This text guides readers through three parts related to domestic and global PHN. It presents a comprehensive survey of where the field has been taken due to the work of Mary Egan and other notable leaders in the field, allowing for groundbreaking new opportunities for practitioners, researchers, policy-makers, and other public health professionals.
KEY CONCEPTS
Public health nutrition, as defined by the Academy of Nutrition and Dietetics Public Health Nutrition Task Force is, “the application of nutrition and public health principles to improve or maintain optimal health of populations and targeted groups through enhancements in programs, systems, policies, and environments”.28
Public health nutritionist, as defined my Margaret Kaufman, is “that member of the public health agency staff who is responsible for assessing community nutrition needs and planning, organizing, managing, directing, coordinating, and evaluating the nutrition component of the health agency’s services … establishes linkages with related community nutrition programs, nutrition education, food assistance, social or welfare services, child care, services to the elderly, other human services, and community-based research”.32
The Social-Ecological Model can be used by public health nutritionists to help them understand the multiple levels of influence on nutrition- and other health-related behaviors. The spheres of influence include:
The individual level, which encompasses age, sex, literacy level, race and ethnicity, food preferences, acute childhood traumas, and more
The interpersonal level, which includes families, friends, social networks, coworkers, and peers
The organizational level, which includes worksites, parks and recreation facilities, early childhood education settings, schools, colleges and universities, and community organizations
Sectors, including governmental, educational, healthcare, transportation, public health, community, and business sectors
Societal and policy levels, such as traditions, beliefs, religions, policies and laws, societal changes, and economic safety nets
The core functions of public health are assessment, assurance, and policy development. There are 10 essential public health services and 16 essential PHN services that support these core functions.
Public health nutritionists should have advanced training in nutrition and public health to develop knowledge of current nutrition-related evidence-based skills related to the core functions of public health and the essential health services of public health and PHN.
CASE STUDY: A PUBLIC HEALTH NUTRITIONIST’S PROCESS FOR INCREASING ACCESS TO HEALTHFUL FOODS IN URBAN AND RURAL COMMUNITIES WITH MOBILE FOOD MARKETS
A public health nutritionist is working with other public health and nutrition professionals on a state coalition to increase access to healthful foods in urban and rural communities. The team begins by assessing the number and types of retail food stores across the state. After finding this information, they then look at the U.S. Department of Agriculture (USDA) Economic Research Service Food Access Research Atlas (www.ers.usda.gov/Data/FoodDesert). They find that many low-income populations in the state have low access to food stores and low vehicle access. Further, the assessment data show that these areas have the highest rates of child and adult obesity and type 2 diabetes. These findings lead the coalition to seek funds for mobile food markets in collaboration with a local food bank and a local grocery store chain. After writing a successful grant application to the Robert Wood Johnson Foundation (www.rwjf.org) and receiving funding, the coalition begins marketing the mobile food markets in eight of the lowest income counties in the state with the lowest access to healthful foods. To reach the most people, the coalition uses social media, provides infographics at the SNAP office (www.fns.usda.gov/snap/supplemental-nutrition-assistance-program) and at area schools and religious organizations, and runs advertisements about the opening day via radio, television, and billboards.
On the opening day, the mobile markets provide low-cost and no-cost healthful foods and beverages to 2,800 families (over 10,000 individuals). In addition, coalition volunteers help eligible participants enroll in SNAP and survey participants to determine barriers and challenges to preparing the foods that the mobile markets carry. The survey results show that participants would like to learn more about how to prepare healthful foods; thus, coalition members contact extension agents in the area to see if they can do cooking demonstrations at the next mobile market via SNAP-Ed and other USDA programs. In addition, they contact the state department of education to propose high school curricular changes that allow students to take nutrition courses that include healthy food preparation methods. Last, coalition members advocate for improved zoning rules in the priority counties to attract full-service grocery stores to the areas.
Case Study Questions
Identify at least 10 essential PHN services described in the case study and categorize them by the associated core functions of public health.
Use the Economic Research Service Food Access Research Atlas to find your home county and determine if there are low-income, low-access areas there.
In what other areas could the coalition advocate to improve food access for the priority communities?
SUGGESTED LEARNING ACTIVITIES
Explore the Association of State Public Health Nutrition website (www.asphn.org) and complete the following:
List the association’s mission and vision.
Describe at least two committees or councils in the association.
List one way you could become involved in the association.
Visit the SNAP website (www.fns.usda.gov/snap/supplemental-nutrition-assistance-program) and find the following:
Based on the website, provide a brief description of SNAP in your own words.
What are the eligibility requirements for SNAP?
What can be purchased with SNAP benefits?
REFLECTION QUESTIONS
Discuss why it is important for public health nutritionists to have advanced training in both nutrition and public health?
This chapter lists several definitions of PHN; compare and contrast these definitions by discussing the commonalities and differences among them.
Describe at least five ways that public health nutritionists can work with other public health professionals to improve population health.
List and describe at least five historical milestone events and/or legislation that led to expanded roles of public health nutritionists in the United States.
Describe the purpose of the World Public Health Nutrition Association.
GLOSSARY
Association of Graduate Programs in Public Health Nutrition:
One of the first formalized organizations for the profession, created in 1950.
Association of State Public Health Nutritionists:
One of the first formalized organizations for the profession, created in 1952.
Practice that relies on scientific evidence for decision-making and informing practice.
Passed by Congress in 1906 to begin oversight of food production, sales, and labeling.
Developed, transitioning, and developing countries have their own unique histories related to the foundations of public health and growth of PHN.
Series of documents that are science-based health objectives for the U.S. population, released every 10 years.
Key descriptors to define PHN:
Solution-oriented, social and cultural aspects, advocacy, disease prevention, and interventions based on systems, communities, and organizations.
Leader in shaping contemporary PHN education and practice in the United States.
Moving to the Future: Developing Community-Based Nutrition Services:
Text providing the delineation of the essential PHN services in relationship to the core functions of public health.
Nutrition and Your Health: Dietary Guidelines for Americans:
Hallmark document providing dietary guidance for the U.S. population that focused on healthful dietary patterns.
Patient Protection and Affordable Care Act:
Legislation that underscores the need for primary prevention as well as screening and treatment of chronic diseases; passed in 2010.
Public health nutritionist:
A member of the public health agency staff responsible for assessing community nutrition needs and planning, organizing, managing, directing, coordinating, and evaluating the nutrition component of the health agency’s services.
Social determinants of health:
Behavioral, environmental, biological, societal, and economic factors that influence individual and population health.
Key model for application by public health nutritionists to understand how behavioral, societal, and economic factors influence health.
Legislation that influenced public health infrastructure and subsequent growth of PHN, passed in 1935.
Special Supplemental Nutrition Program for Women, Infants, and Children (WIC):
One of the first programs to provide nutrition services to pregnant women, infants, and children, established in 1972.
The Future of Public Health:
Groundbreaking document outlining the three core functions of public health—assessment, policy development, and assurance—and the 10 essential services of public health, released by the IOM in 1988.
White House Conference on the Care of Dependent Children:
First conference, held in 1909, by the White House related to PHN.
World Health Organization (WHO):
Created in 1948 as part of the United Nations, formed to combat communicable diseases and to improve maternal, infant, and child health and nutrition.
World Public Health Nutrition Association:
First international organization to promote and improve PHN and to be the international voice of PHN.
REFERENCES
1.
2.
Winslow CEA. The Evolution and Significance of the Modern Public Health Campaign. New Haven, CT: Yale University Press; 1923.
3.
4.
5.
6.
7.
8.
9.
Owen GM, Kram KM, Garry PJ, et al. A study of nutritional status of preschool children in the United States, 1968-1970. Pediatrics. 1974;52(suppl):597–646.
10.
Center for Disease Control and Prevention. Ten-state nutrition survey, 1968-1970. Atlanta, GA: U.S. Department of Health, Education, and Welfare. Publication no. HSM 72-8134; 1972.
11.
Centers for Disease Control and Prevention. National Center for Health Statistics (NCHS).
National Health and Nutrition Examination Survey Data.
History.
2015, November 6.
https://www.cdc.gov/nchs/nhanes/history.htm12.
U.S. Senate Select Committee on Nutrition and Human Needs. Dietary Goals for the United States. 2nd ed. Washington, DC: U.S. Government Printing Office; 1977.
13.
Center for Disease Control and Prevention. Year 2000 national health objectives. MMWR Morb Mortal Wkly Rep. 1989;38(37):629–633.
14.
U.S. Department of Health and Human Services.
Office of Disease Prevention and Health Promotion.
Healthy People.
2019, November 4.
https://www.healthypeople.gov15.
16.
U.S. Department of Agriculture, Agricultural Research Service, Dietary Guidelines Committee.
Report of the Dietary Guidelines Advisory Committee on the Dietary Guidelines for Americans, 1995, to the Secretary of Health and Human Services and the Secretary of Agriculture. Appendix I: History of Dietary Guidelines for Americans.
1995.
https://health.gov/dietaryguidelines/dga95/12DIETAP.HTM17.
Remington PL, Brownson RC. Fifty years of progress in chronic disease epidemiology and control. Morb Mortal Wkly Rep. 2011;60(4):70–77.
18.
Haughton B, Story M, Keir B. Profile of public health nutrition personnel: challenges for population/system-focused roles and state-level monitoring. J Am Diet Assoc. 1998;98(6):664–670.
19.
20.
Probert K. Moving to the Future: Developing Community-Based Nutrition Services. Washington, DC: Association of State and Territorial Public Health Nutrition Directors; 1996.
21.
Hughes R, Begley A, Yeatman H. Consensus on the core functions of the public health nutrition workforce in Australia. Nutr Diet. 2016;73(1):103–111.
22.
23.
24.
25.
26.
Schmidt H. Chronic disease prevention and health promotion. In:
Barrett DH,
Ortmann LH,
Dawson A, et al.
eds.
Public Health Ethics: Cases Spanning the Globe. Cham, Switzerland: Springer;
2016.
https://www.ncbi.nlm.nih.gov/books/NBK435779 27.
28.
29.
30.
Hughes R. Competencies for effective public health nutrition practice: a developing consensus. Public Health Nutr. 2004;7(5):683–691.
31.
Hughes R.
Workforce development: challenges for practice, professionalization and progress.
Public Health Nutr.
2008;
11(8):
765–
767. doi:
10.1017/S1368980008002899 32.
Kaufman M, ed. Personnel in Public Health Nutrition for the 1980’s. McLean, VA: Association of State and Territorial Health Officials Foundation; 1982.
33.
Hughes R.
Definitions for public health nutrition: a developing consensus.
Public Health Nutr.
2003;
6(6):
615–
620. doi:
10.1079/PHN2003487 34.
35.
Strategic Intergovernmental Nutrition Alliance. Eat Well Australia: An Agenda for Action for Public Health Nutrition 2000–2010. Canberra, Australia: Department of Health and Aged Care; 2001.
36.
Rhea M,
Bettles C.
Future changes driving dietetics workforce supply and demand: future scan 2012-2022.
J Acad Nutr Diet.
2012;
112(3):
S10–
S24. doi:
10.1016/j.jand.2011.12.008 37.
Haughton B,
Stang J.
Population risk factors and trends in health care and public policy.
J Acad Nutr Diet.
2012;
112(3):
S35–
S46. doi:
10.1016/j.jand.2011.12.011 38.
. Patient Protection and Affordable Care Act, 42 USC §18001 (2010).
39.
Wells EV,
Sarigiannis AN,
Boulton ML.
Assessing integration of clinical and public health skills in preventive medicine residencies: using competency mapping.
Am J Prev Med.
2012;
42(6):
S107–
S116. doi:
10.1016/j.amepre.2012.04.004 40.
Institute of Medicine.
Who Will Keep the Public Healthy? Educating Public Health Professionals for the 21st Century. Washington, DC: National Academies Press;
2003. doi:
10.17226/1054241.
Bronfenbrenner U.
Toward and experimental ecology of human development.
Am Psychol.
1977;
32(7):
513–
531. doi:
10.1037/0003-066X.32.7.513 42.
Institute of Medicine. Promoting Health: Intervention Strategies from Social and Behavioral Research. Washington, DC: National Academy Press; 2000.
43.
Spence ML, ed. Strategies for Success: Curriculum Guide (Didactic and Experiential Learning). 3rd ed. Association of Graduate Programs in Public Health Nutrition; 2013.
44.
45.
46.
47.
48.
Serra-Majem L.
Moving forward in public health nutrition: the I World Congress of Public Health Nutrition.
Nutr Rev.
2009;
67(suppl 1):
S2–
S6. doi:
10.1111/j.1753-4887.2009.00150.x 49.
50.
Shrimpton R,
Hughes R,
Recine E, et al.
Nutrition capacity development: a practice framework.
Public Health Nutr.
2013;
7(3):
682–
688. doi:
10.1017/S1368980013001213 51.
52.
53.
National Board of Public Health Examiners.
Credentialing Public Health Leaders.
2019.
https://www.nbphe.org54.
55.
Wright K,
Rowitz L,
Merkle A, et al.
Competency development in public health leadership.
Am J Public Health.
2000;
90(8):
1202–
1207. doi:
10.2105/AJPH.90.8.1202 56.
Haughton B,
George A.
The Public Health Nutrition workforce and its future challenges: the US experience.
Public Health Nutr.
2008;
11(8):
782–
791. doi:
10.1017/S1368980008001821 57.
Palermo C,
Hughes R,
McCall L.
An evaluation of a public health nutrition workforce development intervention for the nutrition and dietetics workforce.
J Hum Nutr Diet.
2010;
23:
244–
253. doi:
10.1111/j.1365-277X.2010.01069.x 58.